Recurrence or complications despite medical therapy
Failure or side effects of medical treatment
Patients who do not want to be dependent on medications for the rest of their lives
Very large hiatal hernias (mechanical problems, risk of incarceration)
Long-term patients concerned about the side effects of medication
Patients who want to eliminate the mechanical cause of reflux
Goal of Surgical Therapy
In principle, the mechanical problems that lead to reflux disease can only be solved surgically.
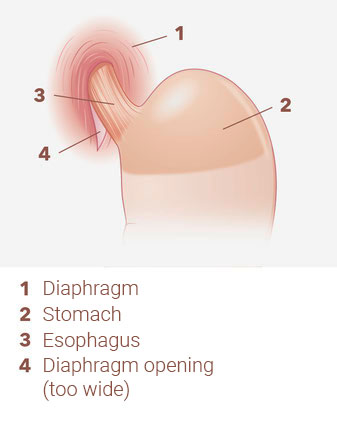
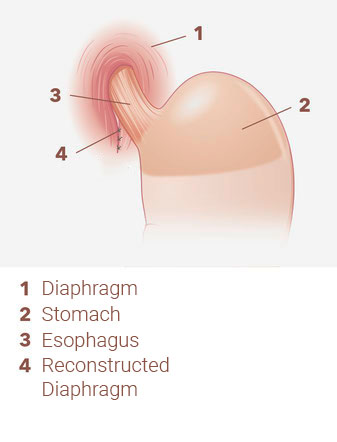
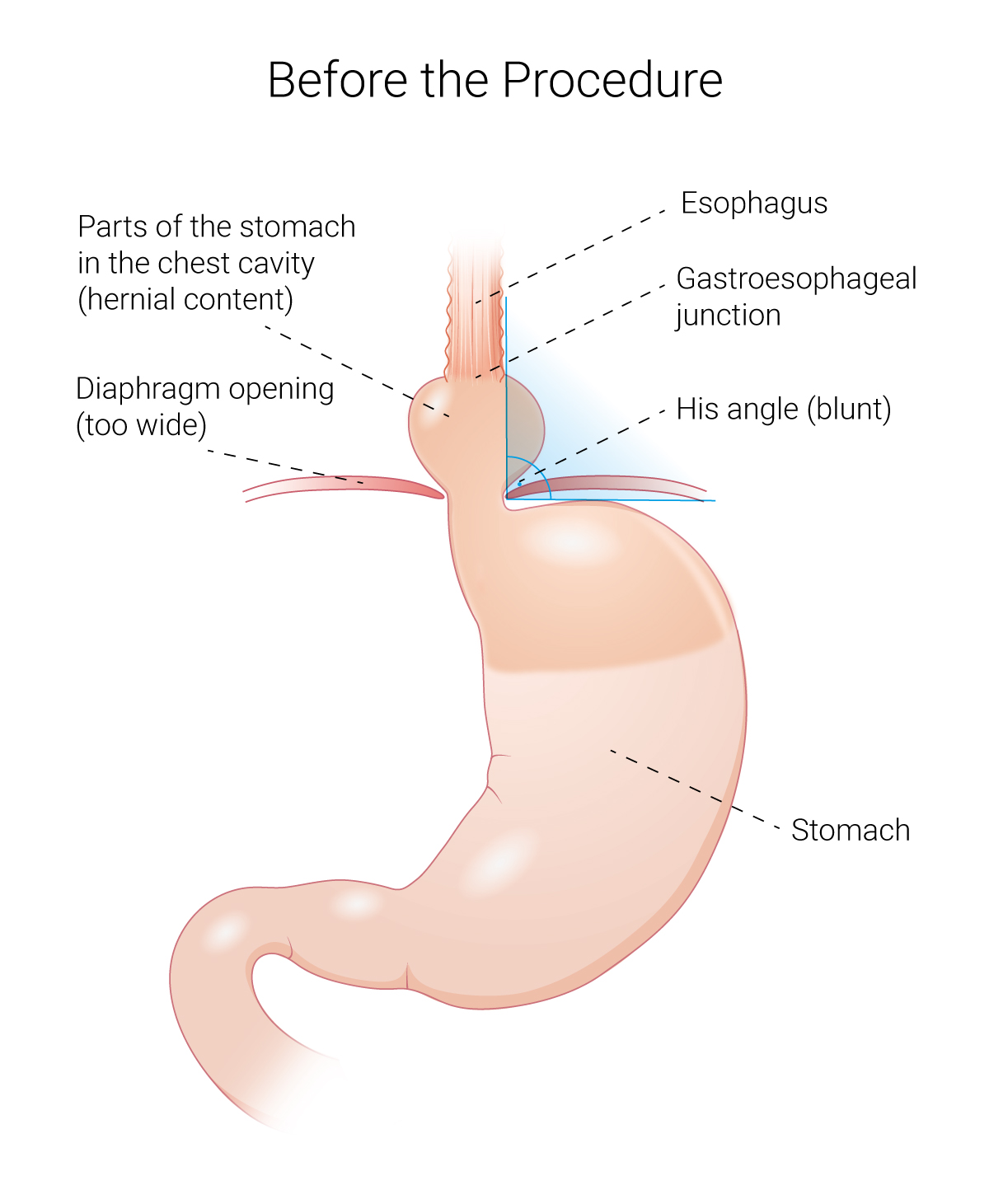
The primary goal of surgery is to move the hernia contents (usually the upper part of the stomach) from the thoracic cavity back into the abdominal cavity. In addition, the enlarged diaphragmatic opening must be reduced in size (see illustrations).
Other surgical steps are then taken to prevent reflux. A variety of procedures are used. Only a few of these have become established. We have divided them into older and modern procedures.
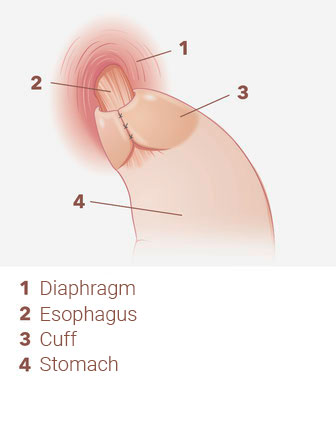
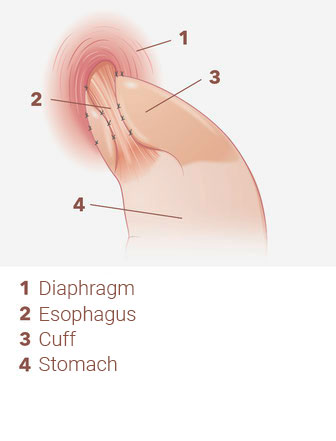
Nissen fundoplication (first described in 1956) and Toupet fundoplication (first described in 1963)
Nissen fundoplication (see illustration) and Toupet fundoplication (see illustration) are classic standard procedures. In both procedures, a gastric cuff is placed around the lowest part of the esophagus (fundoplication). A 360° cuff is used in the Nissen procedure and a 270° cuff in the Toupet procedure. The Toupet procedure has been our preferred procedure for 18 years. The placement of this cuff prevents stomach acid or stomach contents from flowing back into the esophagus.
However, the side effects of “cuffing” can be very unpleasant. As these techniques result in a kind of “valve mechanism”, burping and vomiting are virtually impossible. For these reasons, we practically abandoned these procedures ten years ago in favor of cuffless surgery. Since then, our clearly preferred procedure for the treatment of reflux disease and any diaphragmatic hernia has been our modified BICORN procedure, which we perform exclusively using minimally invasive techniques (see Modern Procedures).
Nissen fundoplication (posterior 360° cuff)
Toupet fundoplication (posterior 270° cuff)
Modern Procedures
BICORN procedure (first performed in 2004, B. Ablassmaier)
The BICORN procedure is an excellent alternative to conventional surgery. The goal of the procedure is to restore normal anatomical conditions. The BICORN procedure does not require the use of a fundoplication.
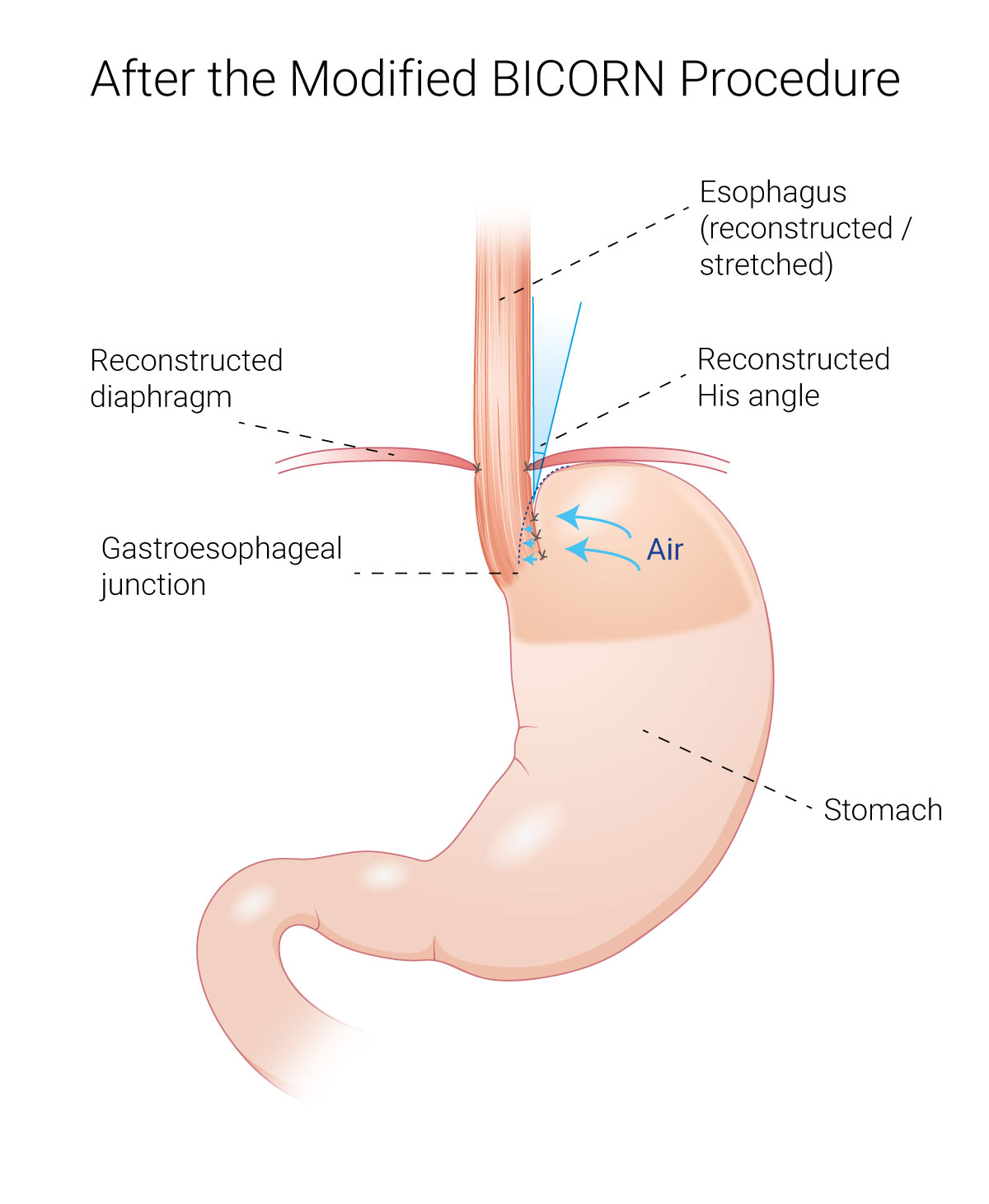
Modified BICORN procedure (first performed in 2014, M. Feigel)
At our center, we have modified the original BICORN procedure by additionally securing the esophagus in its position after surgery. This modified BICORN procedure with simultaneous tension-free fixation of the esophagus to the bilateral diaphragm crura has been our standard procedure for ten years, not least because of the extremely low rate of complications and side effects:
Decisive advantages of the cuff-less procedure:
In contrast to the above mentioned cuff procedures, the patient can burp and also vomit after the modified BICORN procedure. The results in terms of reflux symptoms are absolutely comparable to the cuff procedures.
Principle and mechanism of action:
In the modified BICORN procedure, the upper crescent-shaped part of the stomach is returned to its correct position after surgery. The so-called angle of His is then pointed again (intentionally slightly overcorrected) and no longer blunt (see illustrations). By simultaneously reducing the size of the widened diaphragmatic hiatus and stretching and fixing the esophagus, the normal anatomy and physiology in this area is restored. The pumping function of the esophagus is improved. This simple procedure prevents pathological reflux of acid and stomach contents in the long term.
N.B.
As with all surgical procedures, there is a small risk of recurrence of the hiatal hernia and/or acid reflux. A second operation may be required.
There are some other surgical procedures (e.g. implantation of a special magnetic ring, a silicone cube, esophageal stimulation with electrodes, etc.) that we will not discuss here because we do not recommend or perform them for various reasons.
Own Surgical Experience
We have been performing about 40-50 anti-reflux surgeries per year since 1996 and have a lot of experience in this special surgery. We also perform so-called revision surgeries. These are surgeries that have already been performed to treat reflux disease, but the success of the operation is unsatisfactory or poor. In many cases a new operation (revision) is necessary. Over the past 25 years, we have specialized in these revision surgeries, which can be technically very difficult, complex and not without risk. Our center is known far beyond the borders of the country. Many patients come to us from far away for this unique operation.